Rectal Prolapse
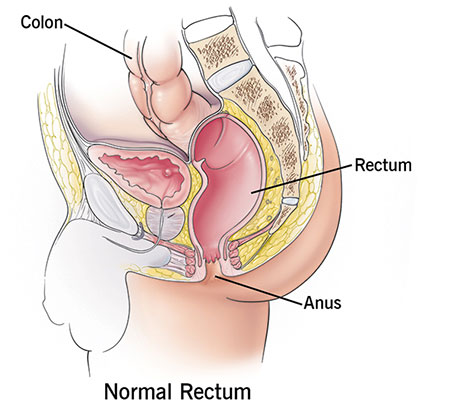
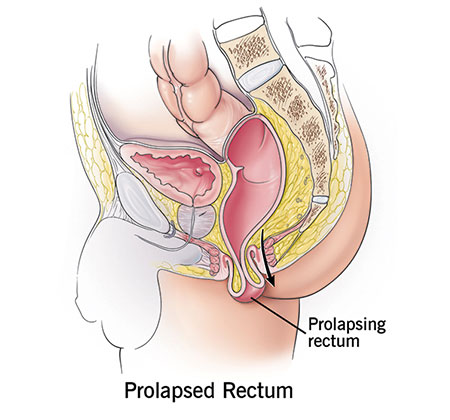
Rectal Prolapse is a condition in which the rectum (i.e. the last few inches of the large intestine) or a part of it, loses its normal attachments inside the body, and protrudes out through the anal opening. Although it is never an emergency problem, it does leave the patient uncomfortable and anxious, with a significant negative impact on the quality of life.
It is more common in females (especially >50 years) than in males.
Causes:
- Long standing constipation with history of straining to defecate.
- Chronic diarrhoea
- Old age - Due to laxity of the pelvic floor muscle and reduced anal sphincter tone.
- Pregnancy, difficult vaginal delivery, multiple vaginal deliveries.
- Chronic cough due to COPD or any other cause
- Neurological conditions like multiple sclerosis, injury to the lower back or pelvis, spinal tumours.
- Cystic fibrosis in children
Symptoms:
- The most common symptom is something lump/ swelling coming out of the anal opening. In the early stages, this may happen only during a bowel movement, but as the condition progresses it may happen on coughing, sneezing and standing up as well.
- Initially it may be possible to push back the swelling inside with your fingers. With time, even this may not be possible and it may persistently stay out.
- In case of Occult prolapse there is no swelling coming out but there may be a sense of incomplete evacuation after a bowel movement, as though something is still left in the rectum.
- Fecal incontinence leading to soiling of clothes. There may be leaking of gas, liquid/solid stools or mucus/ blood stained discharge. The anal sphincter is made of muscles that allow one to hold on to their stool when there is an urge to defecate. When the rectum prolapses, it goes past the anal sphincter, and this allows stools and mucus to pass in an uncontrolled fashion.
- Constipation - Seen in upto 30-50% of patients, constipation may result because of bunching up of the rectum, creating a blockage that worsens with straining.
- Pain/ discomfort in the region.
- With time, the prolapsed mucosa may become thick and ulcerated causing bleeding.
Diagnosis of Rectal Prolapse
A brief clinical history of your symptoms followed by examination of the rectum is done. Your doctor may ask you to strain or cough during the examination. A digital rectal examination is performed followed by Proctoscopy ( visualisation of the rectum by inserting a scope ). Other tests may include :
- MRI Defecography - This test shows how much stool the rectum can hold, how well it can hold and how well it can release the stool.
- Colonoscopy - This is an examination of the large intestine/colon, with the help of a flexible tube that has an inbuilt camera. It is done to rule out any associated condition.
- Anal manometry - This test measures the strength of the anal sphincters, how tightly the sphincters can close.
Types of Rectal Prolapse :
- Partial or mucosal prolapse : Only the inner lining of the rectum protrudes through the anus. It is usually <2cm and produces radial folds.
- Full thickness rectal prolapse / Procidentia : Part of the wall (including all three layers) protrudes through the anus. It is about 2-5cm and produces concentric rings.
- Occult or Internal intussusception : The rectum folds on itself but does not protrude through the anus.
Treatment:
- CONSERVATIVE : Laxatives.
- SURGICAL :
Repair through abdomen.
Laparoscopic Rectal Prolapse Surgery.
Rectal Prolapse repair through anus (Perineal).